


1Dermatology Department, Hospital Clínic & Melanoma Group IDIBAPS (Institut d’Investigacions Biomèdiques August Pi i Sunyer), Barcelona, Spain, 2Medical Sciences Department, Section of Dermatology, University of Turin, Turin, Italy, 3Centro Investigación Biomédica en Red de Enfermedades Raras (CIBERER), Instituto de Salud Carlos III (ISCIII), 4Department of Pathology, Hospital Clínic Barcelona, and 5University of Barcelona, Barcelona, Spain
Sutton naevi can sometimes present a challenging appearance with atypical presentation, also by dermoscopy. Reflectance confocal microscopy could help in making a diagnosis. This study prospectively collected two groups of Sutton naevi: the first one was composed by typical white halo naevi monitored for one year (13, 23%) and the second one was made up of atypical lesions excised in order to rule out melanoma, which were histologically diagnosed as Sutton naevi (21, 37%). These two groups of Sutton naevi were compared to a retrospectively collected cohort of thin melanomas with histologic regression features (23, 40%). On dermoscopy, atypical Sutton naevi and melanomas were indistinguishable. Re?ectance confocal microscopy demonstrated significant differences at the dermo–epidermal junction: marked dermo–epidermal junction thickening and non-edged papilla were associated with melanoma, while the presence of nests was associated with Sutton naevi. However, re?ectance confocal microscopy also detected marked intraepidermal pagetoid cells in Sutton naevi that were a combination of MelanA+ and CD1a+ cells. Sutton naevi can simulate melanoma, under both dermoscopy and re?ectance confocal microscopy. Nevertheless, relevant confocal dermo–epidermal junction features and the clinical scenario can be helpful to make a final diag-nosis, especially in those situations where melanoma must be ruled out.
Key words: Sutton naevus; melanoma; simulator; reflectance confocal microscopy; dermoscopy; dermatoscopy.
Accepted Apr 21, 2020; Epub ahead of print Apr 21, 2020
Acta Derm Venereol 2020; 100: adv00134.
Corr: Cristina Carrera, Dermatology Department, Hospital Clinic Barcelona, Villarroel 170, ES-08036 Barcelona, Spain. E-mail: ccarrera@clinic.cat
Sutton naevi can often be diagnosed easily, but they sometimes present a challenging appearance, without a white halo, clinically and dermoscopically simulating melanoma. Reflectance confocal microscopy, a non-invasive imaging technique that has been demonstrated to improve detection of melanoma, could be used to distinguish these benign inflamed naevi from melanoma. The results of this study show that atypical presentation of Sutton naevi does exist and that, even by re?ectance confocal microscopy, such naevi may be indistinguishable from melanoma. However, the integration of the subject’s age and the careful examination of the dermo-epidermal junction by reflectance confocal microscopy can help clinicians to make the decision between excision or follow-up.
Sutton naevus (SN), also known as halo naevus, is a clinical-pathological condition described by Richard L. Sutton in 1916 as “leukoderma acquisitum centrifugum” (1). SN consists of a benign melanocytic neoplasm with a marked lymphocytic host response, which often leads to regression or involution of the naevus. Clinically, SN usually appears as a central melanocytic naevus surrounded by a symmetrical roundish-to-oval white circle (2).
Although the diagnosis of inflamed melanocytic lesions, such as SN, is usually straightforward (3), some-times inflammation makes these entities suspicious on clinical and dermoscopic evaluation. The atypical features that naevi can present after acute sun exposure and inflammation due to sunburn (4) are also well known. Indeed, inflamed naevi can pose a diagnostic challenge for both clinical and dermoscopic examination, and melanoma has to be ruled out in equivocal cases.
Reflectance confocal microscopy (RCM) is a non-invasive imaging tool that provides an in vivo near-histological horizontal view of the skin. Continuous and substantial development of its applications for the diagnosis of skin conditions has been described during the last decade (5). In particular, RCM evaluation has proven useful in examining clinically and dermoscopically equivocal melanocytic lesions, in differentiating between benign and malignant cases, and thus avoiding unnecessary biopsies of naevi (6, 7).
Dermoscopic differential diagnosis between SN and melanomas can sometimes be a challenge, therefore we suggest that RCM could significantly improve the diagnostic accuracy of dermoscopically atypical inflamed benign naevi, such as SN. The aim of the present study was to describe dermoscopic and RCM features associated with SN, and secondarily, to compare them with inflamed melanomas. A series of SN presented as clinical/dermoscopic atypical lesions, which were excised to rule out malignancy, were compared with a series of classical SN and with melanomas with regression features.
A single-institution prospective cohort of SN was analysed and compared with a historically collected cohort of melanomas.
We collected data from patients referred to the Melanoma Unit at the University Hospital of Barcelona, Spain, between 1 January 2010 and 30 May 2017. The evaluated patients met one of the following inclusion criteria for the 3 groups: (i) dermoscopic atypical melanocytic lesions excised due to the possibility of melanoma, which were subsequently histologically diagnosed as SN; (ii) typical white halo SN; (iii) thin melanomas (Breslow < 1.5 mm) that showed inflammation and regression features on histopathology.
Data regarding the age and sex of the patients, as well as the anatomical location and size of every lesion were collected. Each lesion was documented with a digital camera (Canon PowerShot G10, Canon, Tokyo, Japan) and a high-resolution polarized dermatoscope (DermLite Photo, 3GEN, LLC Dana Point, CA, USA). In vivo confocal microscopy was performed on every lesion with a commercially available reflectance confocal microscope (Vivascope 1500; Lucid Inc., Henrietta, NY, USA), which uses a near-infrared laser at 830-nm wavelength with a maximum power of 35 mW.
Dermoscopy and RCM images were interpreted by consensus by 2 dermatologists. The dermoscopic and confocal criteria used have been described previously in the literature (8–10). Dermoscopic evaluations of the 3 groups were analysed separately. Regarding RCM evaluation, atypical and classical SN were considered as a single group of benign lesions, contrary to melanomas. Histopathological assessment was considered the reference standard for diagnosis of benign (SN) or malignant melanocytic lesions. It was performed by 2 certified dermatopathologists with experience in melanocytic neoplasms. Immunohistochemical studies with mouse monoclonal antibodies against double staining for co-expression Ki67-MelanA (proliferative and melanocyte markers) and for CD1a (Langerhans cell marker) are always performed as routine in our laboratory.
All lesions presenting peripheral symmetrical hypopigmentation (white halo) and no suspicious criteria for malignancy at clinical/dermoscopic examination were defined as clinically typical SN. As a result of the integration of clinical presentation, along with dermoscopic and confocal evaluation, those lesions that were considered SN were not excised and remained under digital monitoring. No suspicious changes were detected after a minimum of 1 year of follow-up.
The Institutional Review Board of Ethics Committee at the hospital clinic approved the protocol. All experiments were conducted in accordance with the principles of the Declaration of Helsinki.
Statistical analyses
For basic statistical analysis, the absolute and relative frequencies of each clinical, dermoscopic and RCM feature were calculated. Fisher’s exact test, χ2-test and Spearman’s correlation coefficients were calculated for each qualitative feature related to the final diagnoses. Student’s t-test was used for quantitative comparison among independent groups. The Kruskal–Wallis test was used for comparison of multiple groups.
Logistic regression was used to examine the association between dermoscopic and RCM features, according to the final pathological report. All statistical tests were 2-sided and a p-value ≤0.05 was considered significant. The analyses were performed by STATA 12 (StatCorp LP, College Station, TX, USA).
Clinical features
A total of 57 lesions from 54 patients were analysed; 21 females (39%) and 33 males (61%). Mean ± standard deviation (SD) age of the entire cohort was 42.6 ± 19.5 years.
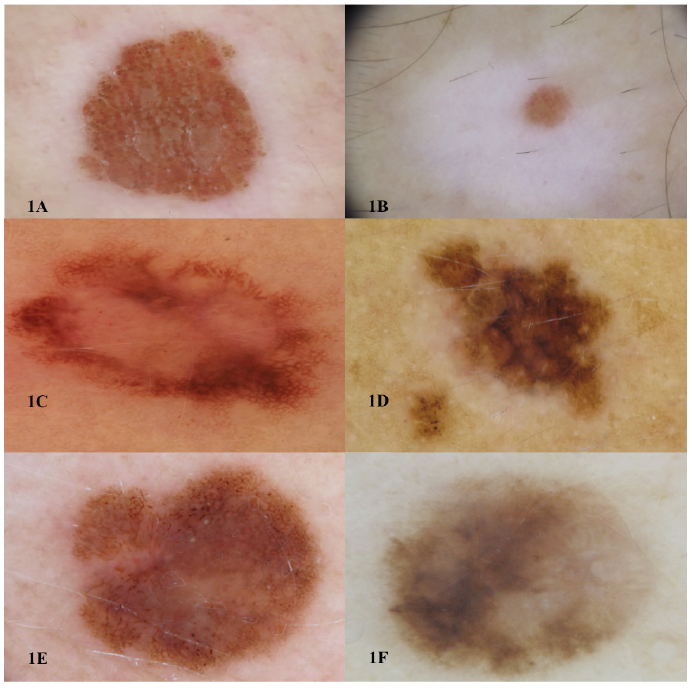
The study included 34 (60%) SN, of which 13 were classical SN (23%), 21 clinically atypical SN (37%) and 23 melanomas (40%) (Fig. 1). Overall, patients with SN were significantly younger than patients with melanoma: 32.1 ± 13.23 years for benign lesions vs. 58.3 ± 16.62 years for melanomas (p < 0.001). No differences between sexes were detected according to malignancy.
Concerning location, 46 lesions (80%) were located on the trunk, 9 (15.8%) on limbs and 2 (3.5%) on the head and neck area. With regard to the diameter of the lesions, benign lesions appeared to be smaller than melanomas; the mean diameter was 5.73 ± 2.76 mm for benign lesions vs. 13 ± 8.72 mm for malignant ones (p < 0.001).
Clinically, 17 lesions had a peripheral whitish halo; of these 16 lesions (94%) were SN, while 1 (6%) was melanoma. Eleven (65%) of the lesions presented a regular and symmetrical halo, in contrast to 6 lesions (including 1 melanoma) in which the halo was irregular and asymmetrical. All lesions presenting with a symmetrical halo were found to be SN.
Fig. 1. Dermoscopic appearance of 6 of the studied lesions. (A, B) Clinically typical Sutton naevi. (C, D) Clinically and dermoscopically atypical presentation of biopsy-proven Sutton naevi. (E, F) Thin melanomas with regression features. Scale: A, C: 8 mm, B: 2 mm, D: 4 mm, E: 12 mm, F: 5 mm.
Dermoscopic features
The main dermoscopic and regression features found in the 3 different groups are summarized in Tables I and II.
The most commonly detected colour was light-brown (n = 29, 51%), followed by dark-brown (n = 20, 35%). Out of the 57 lesions, 18 (32%) presented a global reticular pattern, 17 (30%) a globular pattern, 10 (18%) a reticulo-globular pattern, 10 (18%) a multicomponent pattern, and 2 (4%) a non-specific pattern.
Differences found between clinically atypical SN and melanomas were: the presence of blue-white veil (p = 0.003), streaks (p < 0.01), shiny white streaks (p = 0.03) and blotches (p < 0.01), which were related to malignancy. However, other dermoscopic features that have often been reported to be associated with malignancy (e.g. atypical vessels, ulceration or negative network) did not show statistical differences between atypical presentation of SN and melanomas in our series. The median value of the 7-point checklist was 5 in both groups (atypical SN and malignant melanoma) (Table I).
Table I. Dermoscopic characterization of Sutton naevi and melanomas
Table II. Dermoscopic characterization of regression features
Dermoscopic regression features
Regression was analysed separately according to type (white vs. blue), distribution (peripheral-global vs. central-absent) and percentage within the lesion.
White regression was detected in 43% of atypical SN and in 26% of melanomas (Table II), while blue-grey regression was present in 86% of atypical SN and 61% of melanomas. In terms of distribution, none of the melanomas presented peripheral/global peppering, in contrast to 19% of the atypical SN (p = 0.028).
Reflectance confocal microscopy features
Confocal features are summarized in Table III. In the epidermis, the presence of atypical pagetoid cells and tangled lines (suggestive of dendrites) were seen in both atypical SN and melanomas (60% and 65%, respectively) (p = 0.3 and p = 0.5). Roundish pagetoid cells were found in 33.3% of atypical SN and 47.8% of melanomas (p = 0.1).
Table III. Characterization using reflectance confocal microscopy
At the dermo–epidermal junction (DEJ), the presence of nests was associated with benign lesions (p = 0.03), while melanomas presented a higher prevalence of junctional thickenings compared with SN. Presence of at least 10% junctional thickenings was significantly related to melanoma (p = 0.04). None of the studied melanomas showed less than 10% junctional thickenings. The presence of at least 10% non-edged papilla was significantly higher in melanomas compared with SN (p = 0.03). Neither the presence of junctional ringed pattern nor the presence of more than 50% of atypical basal cells significantly differed between benign and malignant lesions. However, the presence of dendritic atypical basal cells was observed in 70% of melanomas and in 42% of benign lesions (p = 0.04). Moreover, the presence of roundish basal cells was significantly related to malignancy (83% of melanomas vs. 48% of SN, p = 0.01).
Concerning dermal findings, overall a high proportion of lesions presented features compatible with inflammatory phenomena (76% plump cells and 87% bright particles). Both SN and melanomas presented nucleated atypical dermal cells, plump cells and bright particles, and none of the evaluated features were statistically related to whether the lesion was benign or malignant (Fig. 2).
Fig. 2. Sutton naevus. A 16-year-old male patient with familial history of melanoma and multiple atypical naevi, with a growing lesion on his back. (A) Asymmetrical atypical pigment network and blotch on dermoscopy. (B, arrows) Reflectance confocal microscopy section at the epidermis showing numerous dendritic pagetoid cells. (C, arrows) Non-edged papillae and junctional thickenings at the dermal-epidermal junction. (D, arrows) Atypical nucleated cells on basal layer and dermal papillae. (E) Histopathology revealed compound naevus with dense lymphocytic infiltrate in the dermis, compatible with Sutton naevus. A: Dermoscopy image (5 mm), B–D: Confocal mosaic (B: 1 x 1 mm, C: 1.5 x 1.3 mm, D: 0.75 x 0.75 mm), E: Hematoxilin-eosin (x40).
All 57 tumours were histopathologically reviewed and diagnosis was reached by consensus between 2 expert dermatopathologists. The tumour board meeting formed by experts in the field of melanoma, dermoscopy, confocal microscopy and dermatopathology agreed the confocal-histopathological correlations. Immunohistochemical studies (Melan A and CD1a antibodies) demonstrated that the atypical intraepidermal and basal cells seen in SN by RCM corresponded to a combination of large melanocytes and Langerhans cells (Fig. 3) occupying the epidermis and DEJ.
Fig. 3. Sutton naevus. Reflectance confocal microscopy (RCM) and immunostaining correlation of pagetoid cells. (A) RCM single image (500×500 μm) at the subcorneal layer; several dendritic pagetoid refractile cells are observed (arrows). (B) RCM single image (500×500 μm) at intraepidermal layer (deeper than A), atypical cobblestone pattern with multiple dendritic refractile cells are detected (arrows). (C) Histopathological slide (200×) with CD1a immunostaining identifying Langerhans cells (arrows) infiltrating the epidermis and follicular infundibulum. When evaluating papillary dermis these CD1a positive cells are organized in nest-like structures.
Evaluation of intensely inflamed naevi, such as SN, poses a diagnostic challenge, since they can present with both atypical dermoscopic and confocal findings. The main confocal features usually associated with melanoma, such as intraepidermal pagetoid dendritic and roundish cells and atypical nucleated cells at the basal layer or within the dermal papillae, were all, to some extent, found in the present series of SN.
The current study found that some SN share atypical dermoscopic and confocal features with melanomas; therefore, the distinction between both entities in daily practice is complicated. As an example, the median value of the 7-point checklist was 5 in the group of atypical SN, and the same value was seen in the melanoma group; this illustrates the degree of atypical dermoscopic presentation that SN can show and the difficulties for clinicians in assessing these types of lesions with dermoscopy.
It is important to keep in mind that this atypical presentation of SN is extraordinary. To give a general overview, in our referral department, approximately 240 naevi with some degree of dysplasia and 140 melanomas are excised per year. This means that atypical SN could represent less than 1.4% of atypical benign naevi excised.
According to the literature (11), the age of patients is an important clinical marker of risk. In the current series, patients with SN were significantly younger than melanoma patients.
It is well accepted that melanocytic lesions with extensive regression features should be considered suspicious, especially if regression is seen in more than 50% of the entire lesion. The fact is that regression is seen in both atypical SN and melanomas (12, 13). Moreover, regression is a suspicious sign, which often leads to excision, even though it is difficult to differentiate between benign and malignant lesions using this feature alone. In the current study, we were able to find some differences relating to the distribution of the regression in the lesion. In fact, we found that, although atypical SN and MM can both present white and blue-grey regression, none of the melanomas in the current study presented peripheral/global peppering, in contrast to 19% of the atypical SN (p = 0.028). This may be related to the differences found in the underlying immune reaction developed in the subset of inflamed benign lesions (Meyerson or SN) in contrast to the inflammation seen in malignant lesions (14). There can be a mixture of Meyerson’s and also Sutton’s types of inflammation in the same patient (15), which can lead to more atypia (16, 17).
The main role of confocal microscopy (RCM) in patients with multiple naevi is to increase specificity with-out losing sensitivity in order to detect early melanomas, therefore avoiding excision of typical naevi (6). The confocal findings in the current study can be used to differentiate between benign and malignant lesions, and are useful to characterize lesions in terms of percentage and distribution of RCM parameters. In particular, the presence of at least 10% of junctional thickenings, at least 10% of non-edged papilla and atypical basal cells are the findings associated with diagnosis of melanoma.
When comparing SN with melanomas with regressive features, we observed the most specific confocal features previously reported for melanoma were found in both groups: both SN and melanomas could present atypical dendritic and round pagetoid cells infiltrating the epidermis, atypical basal cells, disarranged dermo–epidermal architecture and atypical nucleated cells within dermal papillae.
Regarding RCM, we realized that looking at epidermal and dermal mosaics (Vivablocks), SN can be equivocal due to an important presence of pagetoid cells in the epidermis and a strong infiltrate of plump cells with bright particles in the dermis (Fig. 2). These findings can be related to the presence of epidermal Langerhans cells or inflammatory infiltrates (3), and these usually prompt clinicians to perform an excision of the lesion, since these features have often been reported in melanomas. In fact, the main confocal features included in melanoma algorithms (6, 18) are the presence of atypical pagetoid cells, non-edged papillae and atypical junctional or dermal cells. This clearly demonstrates the importance of these RCM features when evaluating lesions. The present study demonstrated that the atypical cells seen in SN by RCM correspond to Langerhans cells (CD1a+) and also to atypical melanocytes within the epidermal and basal layers (Melan A+). Therefore, SN should be considered as a possible false-positive (melanoma simulator) by confocal evaluation.
To summarize the RCM findings, the most significant differences between SN and melanoma were related to DEJ architecture. The presence of at least 10% of junc-tional thickenings, at least 10% of non-edged papilla, and atypical basal cells (either dendritic or roundish), were the findings associated with malignancy, while the presence of nests was more related to benignity. No differences were found regarding epidermal RCM features evaluated as SN can present marked pagetoid intraepidermal cells similar to those seen in melanomas.
Study limitations
This is a single-centre study, and the limited sample size might have impacted on its power. Also, most of the clinically typical halo SN were not excised, and therefore were not evaluated by histopathology. How-ever, they were systematically monitored clinically, dermoscopically and by RCM examination and neither relevant changes nor suspicious criteria were detected after 12 months’ follow-up. Evaluation of dermoscopic and RCM images was performed by consensus between 2 readers, rather than independently performed. Confocal limitations in depth did not allow proper evaluation of deep dermis. Furthermore, the vascularity of every lesion was not taken into account, since the study did not record video-files examining blood vessels by RCM.
Conclusion
This study demonstrated that a certain rare group of SN can have dermoscopic and RCM features that make them indistinguishable from melanoma and, as a consequence, they should be removed in order to avoid the possibility of malignancy. However, RCM examination can be helpful if it detects less than 10% of non-edged papillae, less than 10% of junctional thickenings, or the presence of nests at DEJ, as these are features indicative of a benign lesion. Finally, this study confirms that the age of the patient is a robust factor in deciding to excise an inflamed atypical lesion in adulthood. In conclusion, SN can present as melanoma simulators (false-positives) by RCM; therefore the integration of clinical findings with dermoscopic and confocal findings is necessary in order to make final decisions regarding excision or follow-up.
The authors thank all members of the Dermatology Department of Hospital Clinic and the Melanoma Group of IDIBAPS, Barcelona, who participated in visiting patients and taking images of all cases. We thank the study nurse and the technician team; Beatriz Alejo, Pablo Iglesias, Abel Caño, Mireia Domínguez, Daniel Gabriel, M Eugenia Moliner. We especially thank Paul Hetherington, PhD, for his assistance in English editing of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize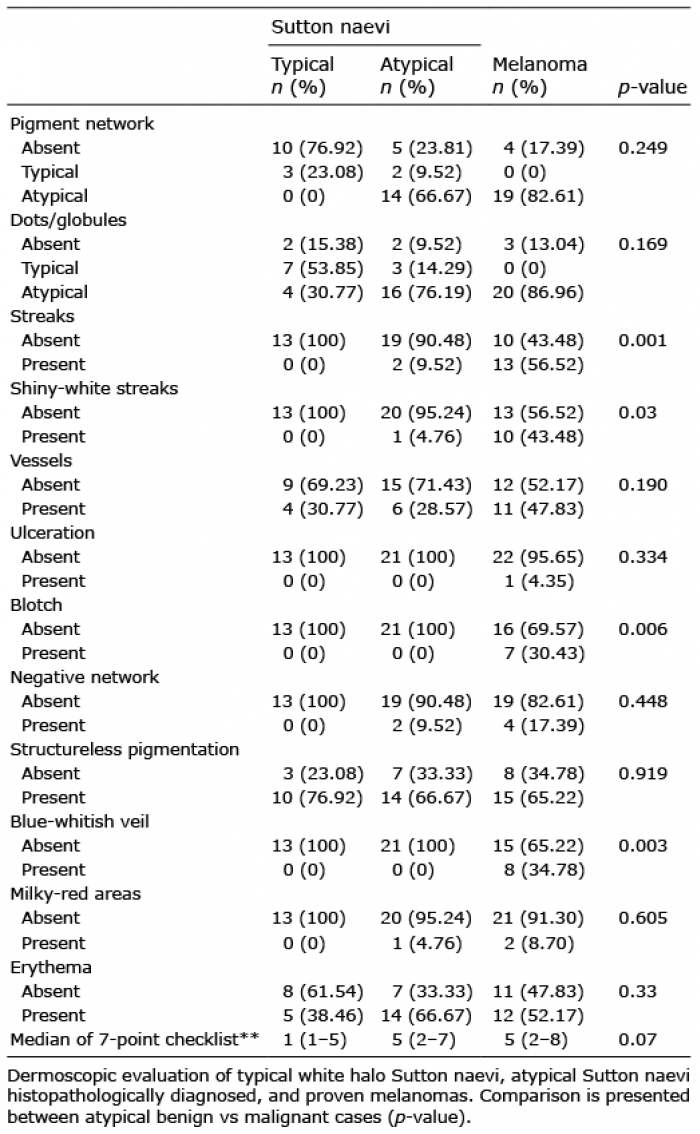 Click to show fullsize
Click to show fullsize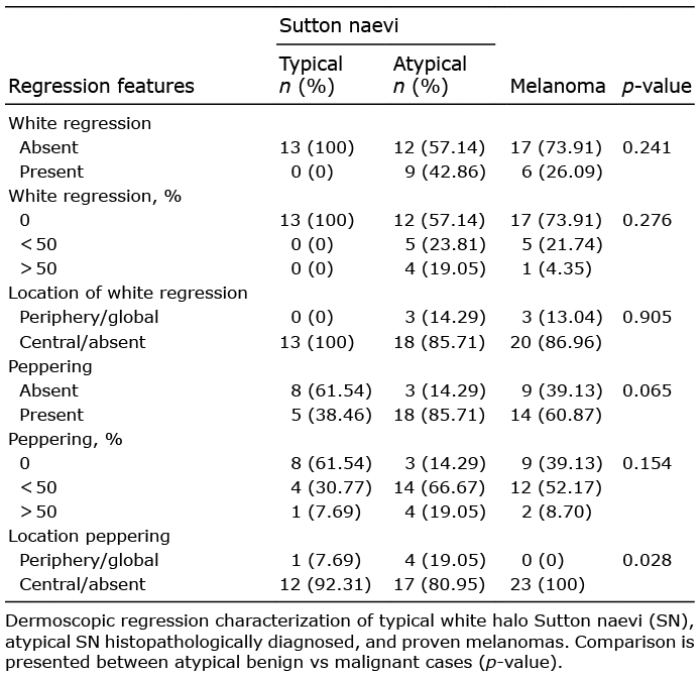 Click to show fullsize
Click to show fullsize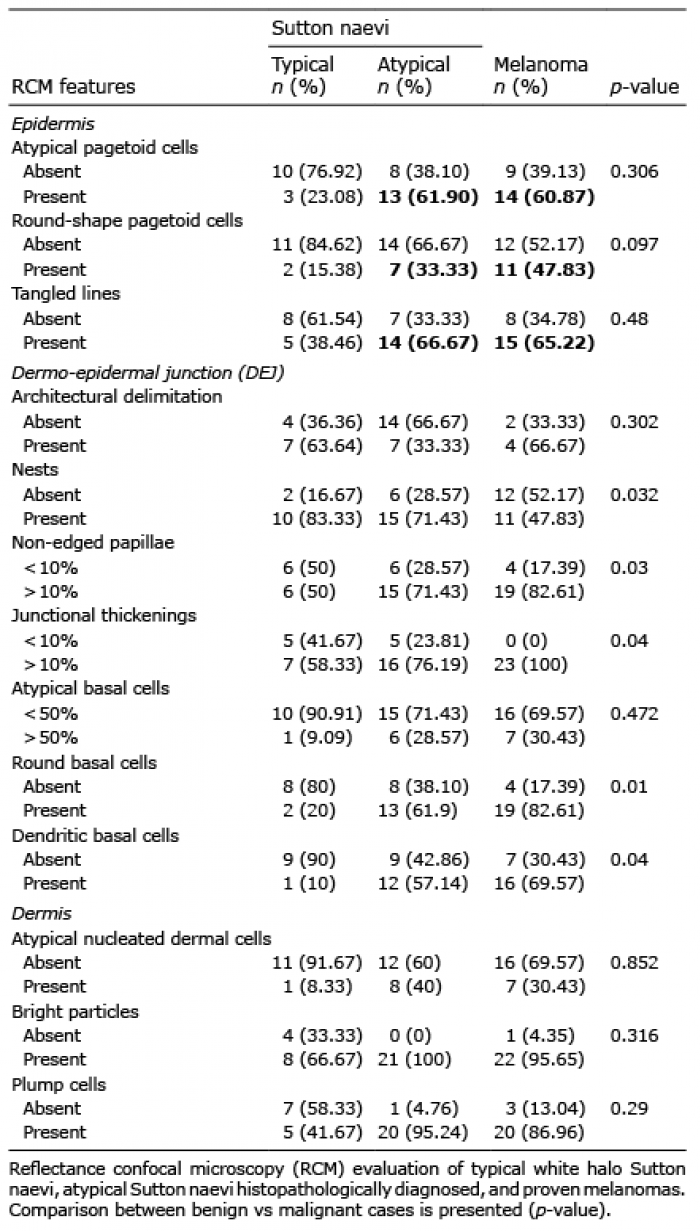 Click to show fullsize
Click to show fullsize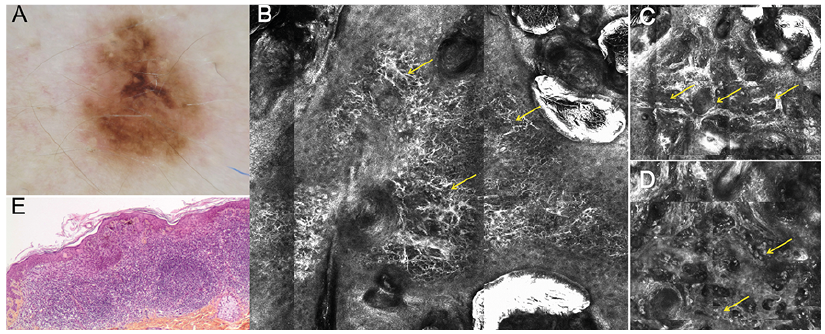 Click to show fullsize
Click to show fullsize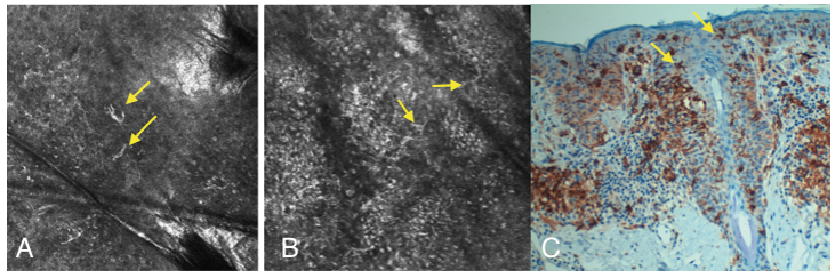 Click to show fullsize
Click to show fullsize